Relationship between lifestyle and mental health over the life course
- A health-supporting lifestyle is associated with better mental health and well-being throughout the life course.
- Both lifestyle and mental health indicators reveal systematic demographic and socioeconomic inequalities. Vulnerable population groups are more frequently exposed to health-damaging lifestyles and mental health problems.
- The approach to improving mental health and well-being must be holistic, taking into account social context and environmental factors as well as individual lifestyle.
The life course covers all the stages of a person’s life from birth to death, and although the trajectory of each life as a whole is ultimately different, the challenges presented by the different stages of the life course are similar for everyone. The different stages of life are also sequentially connected: the starting point for adulthood depends to a great extent on childhood and adolescence while the outcomes in old age can be seen as a result of the person’s experiences during adulthood. The cumulative effects of the life course also apply to health, which in the broadest sense may be defined as physical and mental equilibrium and integrity.
This chapter combines the life course perspective and the social health determinants approach. The four articles in this chapter provide an overview of the associations between lifestyle and mental health in Estonia and their changing patterns. The following brief introduction covers some possible explanations for the associations between lifestyle and mental health, describes the methods and databases used in the articles, and summarises the main findings.
Looking at health and its determinants from the life course perspective allows us to understand health trajectories and describe the development of certain behavioural patterns and health risks.
Although the scientific literature on health effects across the life course is rich and varied, three major approaches can be distinguished. The first is the critical period hypothesis, which focuses on early life (and prenatal) factors. During this period, the child is particularly vulnerable, and factors and risks that inhibit development can have a lasting effect on health. The second approach is the cumulative exposure hypothesis, which rests on the idea that most chronic health conditions develop over a long period of time and that the majority of health outcomes are not the result of early exposure but rather the combined impact of factors accumulated throughout life. These two approaches are combined in a third one, the social trajectory hypothesis, which stipulates a chain of connections between childhood exposure and adult exposure, with only the latter directly affecting morbidity risk. This last model offers hope that interventions in adulthood can mitigate health damage incurred in childhood and that the adjustment of behavioural factors can change the risk of future illness.
In broad terms, health determinants are distributed between the areas of lifestyle, environment, genetics and the healthcare system (Lalonde 1981), individuals have the most control over the health effects of their lifestyle. Depending on the decisions and choices a person makes, a lifestyle may or may not be health-supporting (Tulchinsky 2018). The lifestyle-shaping decisions people make in turn exist in a wider framework of psychosocial, community-specific, socioeconomic and social context-related factors. These have been described by Göran Dahlgren and Margaret Whitehead in their illuminating 1991 model of the main health determinants (Dahlgren and Whitehead 2021) (Figure 2.0.1).
Figure 2.0.1. Main health determinants
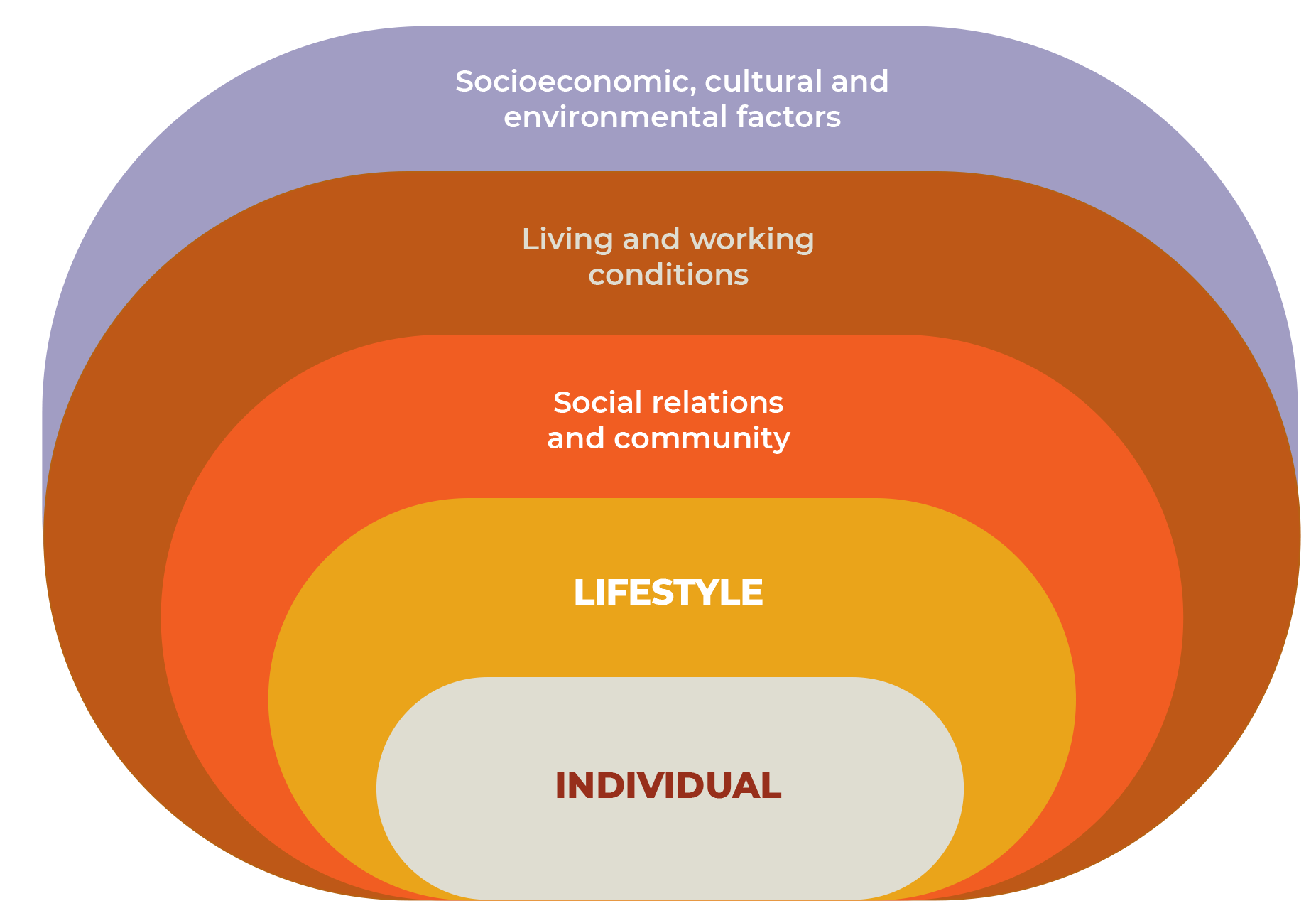
Source: figure adapted by authors (Dahlgren and Whitehead 2021).
The primary starting point for understanding the relationship between lifestyle and mental health is emotions. Usually understood as affective mental states, emotions are complex processes that involve changes in human physiology, subjective experience and its behavioural expression. What interests us here is the role of emotions in making choices that directly affect health. Behavioural decisions are often shaped by emotionally charged situations (Ferrer and Mendes 2017). examples include speeding, alcohol abuse, unprotected sexual intercourse and other similar situations. This knowledge is also successfully utilised by the advertising industry, which often uses positive emotions and feelings to downplay the risks associated with health-damaging products. The relationship between emotions and health outcomes is also apparent in the context of morbidity. For example, negative emotions can increase susceptibility to illness (Everson-Rose and Lewis 2005) and the stress that comes with experiencing illness can influence the course of the illness through both health behaviour and treatment adherence.
Scientific literature associates daily activities, life events, role overload or conflict with the experience of social stress (Gerhardt et al. 2021), which can manifest as anxiety, depression and other mental health problems (Kubzansky et al. 2015).
In addition to causing physiological and neurobiological changes (Godoy et al. 2018) stress has a role in shaping various behavioural responses. Scientific research provides plenty of examples of how high stress levels are associated with diet and excess weight as well as an increase in risk behaviour (Ceccato et al. 2016; Scott et al. 2012)
Another related concept is health inequality, which refers to the existence of systemic differences in health outcomes favouring one group over another based on some feature of the social background. By its very nature, health inequality is a universal and unfortunately inevitable phenomenon whereby a lower social position usually correlates with poorer health indicators.
Knowledge, money, power, contacts and skills are all useful capital that can be employed to avoid health risks or reduce harm. When these resources are scarce, the question of choice becomes the question of opportunities. Manifestations of health inequality can also be explained through behavioural rationale, as the norms and habits specific to different population groups directly shape different lifestyle practices and thereby lead to different health outcomes. n the other hand, the available evidence also unequivocally indicates that the accumulation of factors related to an unfavourable social status increases the risk of health-damaging behavioural patterns and reduces the likelihood of behavioural change. Similar socioeconomic patterns emerge in mental health: lower social status increases the likelihood of experiencing more negative life events (e.g. job loss), having more chronic social stressors (e.g. uncertainty about maintaining a job) and experiencing discrimination. It is important to consider that
from a life course perspective, these risks are not discrete but cumulative. Therefore, seemingly personal emotions and lifestyle choices may stem from external factors largely determined by the surrounding environment.
The model of the main health determinants (Dahlgren and Whitehead 2021) outlined above combines different perspectives on the biological, psychological and social factors of (mental) health and is key to understanding the relationship between lifestyle and mental health in different stages of the life course.
This chapter explores the relationship between lifestyle and mental health and wellbeing in four articles focused on the different stages of the life course.
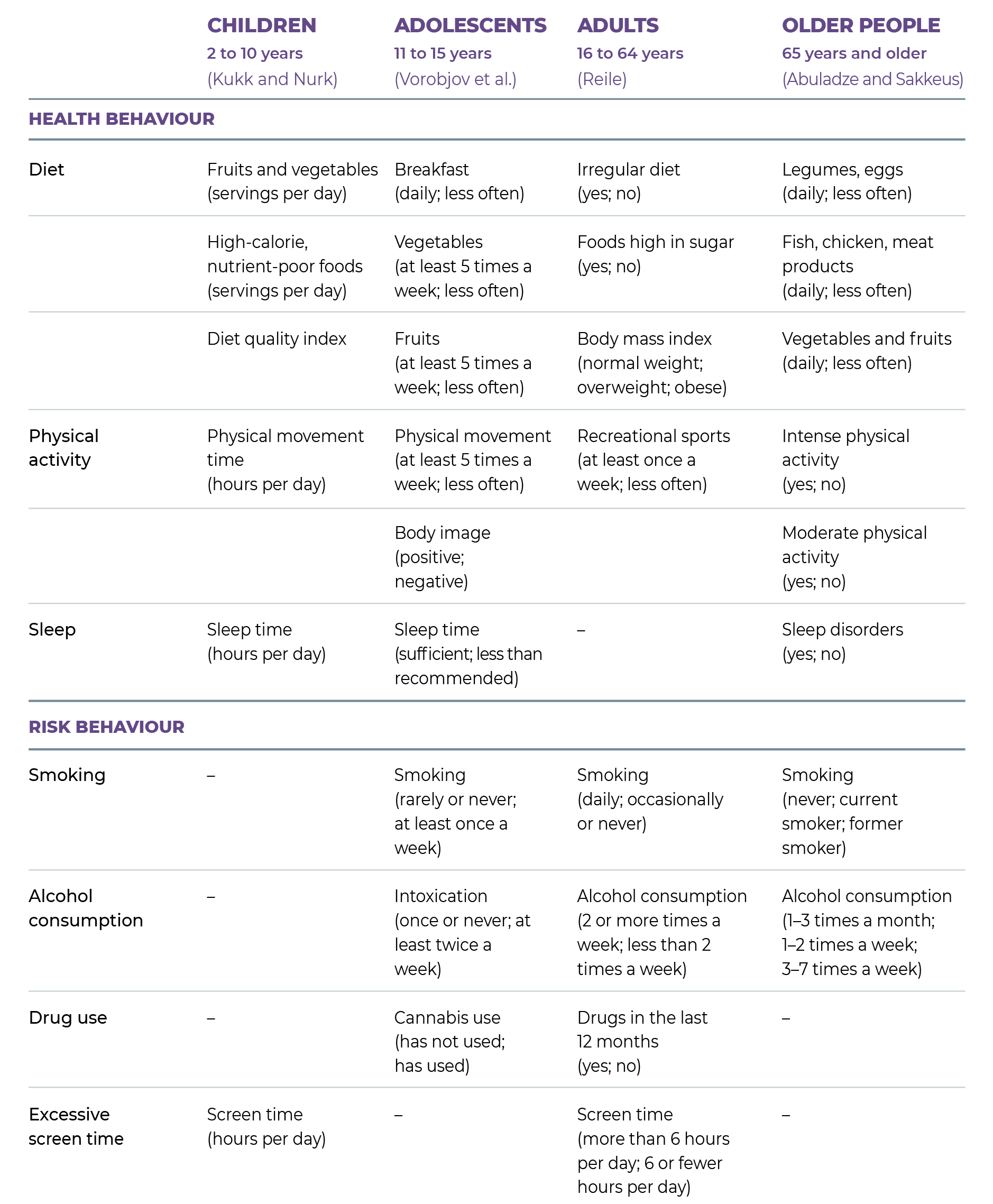
The line between health and risk behaviour can sometimes become fuzzy and depends on the specific context; for example, a poor diet or modest physical activity can also be considered risk behaviour. Due to the availability and different attributes of the underlying data, approaches to indicators of health behaviour and risk behaviour in the articles also vary (Table 2.0.1).
The articles focus on the various aspects of mental health, such as the subjective well-being index, emotional well-being, sadness and depressive symptoms, depressiveness, self-reported stress, fatigue and suicidality. Depending on their respective datasets, the articles describe how trends in the relationship between lifestyle and mental health and well-being have changed over the years, compare Estonian mental health indicators with those of other countries, and highlight mental health inequalities between different population groups. The relationship between mental health and lifestyle factors is modelled mainly by using logistic regression, the common method for analysing cross-sectional data. To simplify, an odds ratio (OR) represents the different odds of an outcome (e.g. mental health problem or level of well-being) occurring depending on the presence of different background variables (e.g. health-supporting behaviour, risk behaviour).
The empirical parts of the articles rely on data from population-based surveys conducted in Estonia between 1990 and 2022. The article on children’s well-being and lifestyle uses data from the 2013–2015 Estonian National Dietary Survey on children aged between 2 and 10 years, which relies on statements by parents. The article on the relationship between young people’s lifestyle and mental health draws on the datasets of the six waves of the Health Behaviour of School-aged Children (HBSC) study in Estonia, which took place from 2002 to 2022 and was targeted towards children aged 11, 13 and 15. The analysis of mental health and lifestyle factors in adults is based on the Health Behaviour among the Estonian Adult Population survey conducted between 1990 and 2020 on the population aged 16 to 64. For older people (65 years and older), the 2013 data of the SHARE survey is used.
Summary
A health-supporting lifestyle is associated with better mental health and well-being throughout the life course. The importance of lifestyle for mental health is most apparent among young people and adults. Parents rate the mental health of Estonian preschool- and primary-school-aged children as quite good, but children’s subjective mental well-being decreases with age. However, it is worth remembering that well-being assessments made by parents are mostly biased in a more positive direction. Over the past decade, mental health problems have increased among young people and remained fairly stable among adults. In older people, mental health issues are significantly associated with pre-existing health problems and limitations. In addition, the comparisons drawn in the articles about young people and older people show that mental health indicators in Estonia are poorer than in several other European countries. In adults, socioeconomic inequalities are reflected in both lifestyle and mental health indicators, and the accumulation of factors related to an unfavourable socioeconomic status and health-damaging lifestyle increase mental health vulnerability. The lifestyle choices of children and young people, on the other hand, are largely shaped by their parents, in leading by example, setting rules and holding joint family activities.
Selecting source material for the articles was demanding, as it was difficult to find directly comparable datasets that would cover the entire course of life. As a compromise, lifestyle and mental health were studied using data from different years and addressing different questions. In many cases, these forced choices made it difficult to interpret the relationship between lifestyle and mental health from a life-course perspective. On the other hand, the solution presented in this chapter offers a unique view of the recurrence of lifestyle and mental health patterns in different stages of life.
The first thing that each person can do for their mental health is to pay attention to their lifestyle choices and keep them balanced and sensible.
Ceccato, S., Kudielka, B. M., & Schwieren, C. (2016). Increased risk taking in relation to chronic stress in adults. Frontiers in Psychology, 6(JAN), 2036. https://doi.org/10.3389/FPSYG.2015.02036/BIBTEX
Dahlgren, G., & Whitehead, M. (2021). The Dahlgren-Whitehead model of health determinants: 30 years on and still chasing rainbows. Public Health, 199, 20–24. https://doi.org/10.3389/fpsyg.2015.02036
Everson-Rose, S. A., & Lewis, T. T. (2005). Psychosocial factors and cardiovascular diseases. Annual Review of Public Health, 26, 469–500. https://doi.org/10.1146/ANNUREV.PUBLHEALTH.26.021304.144542
Ferrer, R. A., & Mendes, W. B. (2017). Emotion, health decision making, and health behaviour. Https://Doi.Org/10.1080/08870446.2017.1385787, 33(1), 1–16. https://doi.org/10.1080/08870446.2017.1385787
Gerhardt, C., Semmer, N. K., Sauter, S., Walker, A., de Wijn, N., Kälin, W., Kottwitz, M. U., Kersten, B., Ulrich, B., & Elfering, A. (2021). How are social stressors at work related to well-being and health? A systematic review and meta-analysis. BMC Public Health, 21(1), 1–17. https://doi.org/10.1186/S12889-021-10894-7/TABLES/5
Godoy, L. D., Rossignoli, M. T., Delfino-Pereira, P., Garcia-Cairasco, N., & Umeoka, E. H. de L. (2018). A comprehensive overview on stress neurobiology: Basic concepts and clinical implications. Frontiers in Behavioral Neuroscience, 12, 127. https://doi.org/10.3389/FNBEH.2018.00127/BIBTEX
Kubzansky, L. D., Winning, A., & Kawachi, I. (2015). Affective states and health. Social Epidemiology, 320–364. https://doi.org/10.1093/MED/9780195377903.003.0009
Lalonde, M. (1981). A new perspective on the health of Canadians.
Scott, K. A., Melhorn, S. J., & Sakai, R. R. (2012). Effects of Chronic Social Stress on Obesity. Current Obesity Reports, 1(1), 16. https://doi.org/10.1007/S13679-011-0006-3
Tulchinsky, T. H. (2018). Marc Lalonde, the Health Field Concept and Health Promotion. Case Studies in Public Health, 523. https://doi.org/10.1016/B978-0-12-804571-8.00028-7